The REAL Truth About Pain Science & Body Mechanics: A Response to Criticism

Joel Seedman, a personal trainer, recently wrote an article called the The Truth about Pain Science and Biomechanics, which presents a lengthy attack on “pain science experts.” Seedman claims they spread dangerous misinformation about the connection between movement and pain, including that pain is all in your head, that injuries or tissue damage don’t matter for pain, that there are no wrong and right ways to move, and that even athletes and heavy weightlifters shouldn’t worry about moving with good technique to protect themselves, even when high levels of force are involved.
Regular readers of this blog, and anyone familiar with the pain science community, will quickly recognize that these claims are very obviously not true. But the article may be persuasive to those with less exposure to the subject matter. Following is a detailed response, geared toward people who are not familiar with the work of pain science educators like Lorimer Moseley, David Butler, Adrian Louw, Peter O’Sullivan, Greg Lehman or Ben Cormack. For those who are, this article might serve as a convenient reference or link in debates on social media.
Quick summary
Seedman’s post is extremely long, but boils down to a few major claims, which I answer in brief in this section and in more detail below.
Claim 1
Seedman claims pain science experts teach that pain is “all in your head,” and that people shouldn’t worry about tissue damage, injury, and movement technique. These are straw men arguments, and it is telling that Seedman doesn’t identify any specific individuals or quotes. The truth is that pain scientists don’t say these things and frequently disclaim them. See below for many examples.
Claim 2
Seedman claims pain scientists misinterpret MRI studies showing that high percentages of people without pain have significant tissue damage such as herniated discs, torn rotator cuffs and degenerative changes in joints. Seedman claims these people will surely have pain in the future. However, several studies have found that MRI results for asymptomatic people have little or no ability to predict future pain, even after five or ten years.
Claim 3
Seedman claims pain scientists have misinterpreted the research showing poor correlations between pain, posture, and “dysfunctional” movement patterns. The studies cited by Seedman are cherry picked, and run against the overall weight of the evidence, which is shown with a fuller examination of the research. Posture and habitual movement patterns are not irrelevant for pain, but have been massively overemphasized in common practice.
Claim 4
Seedman claims pain scientists misunderstand the role of inflammation in pain, which is supposedly the key link between aberrant movement and pain. This is a strange claim, as the role of inflammation in pain sensitivity is one of the most basic aspects of pain physiology. Although chronic inflammations is clearly related to bad health and reduced function, there is no evidence it is caused by bad posture or movement patterns.
Claim 5
Pain science education has only a moderate effect on reducing pain, and the mechanism of effect may be getting people to move more. This is a defensible claim, but not inconsistent with the view of pain educators, who uniformly agree that we don’t have any magic bullets for chronic pain, and that it can be a difficult problem to resolve.
Here’s more detail on the above arguments, supported by extensive citation to authority.
1. Pain scientists do not teach that pain is all in your head
Seedman’s article attacks “pain scientists”, but does not identify specific people or books. However, he seems to be referring to educators who teach basic pain physiology to physical therapists, chiropractors, bodyworkers, and personal trainers. The goal of this education is to help practitioners improve their treatments, and to explain to their clients why they hurt, so they can take an active role in recovery.
The most popular source of information about pain science is the book Explain Pain and associated courses, from Lorimer Moseley (pain scientist and physical therapist) and David Butler (physical therapist and education specialist). Another well known educator is Greg Lehman, a physical therapist, chiropractor and former biomechanics researcher who studied under Stu McGill. Lehman teaches a course called Reconciling Pain Science and Biomechanics, and his free workbook can be found here. I have attended all these courses, teach similar courses occasionally, speak at pain science conferences, and recently published a book called Playing With Movement which addresses similar topics. So I have direct experience with the message that pain educators are trying to send. Here are some of the major points that we think its important for people to understand:
- Pain is multi-factorial and “biopsychosocial.” It depends on peripheral factors like tissue damage, injury and inflammation (that’s the bio part), but also perceptions, thoughts, emotions, and social stress (that’s the psychosocial part). It is also complex, meaning these different factors interact in ways that are often individual, context-dependent, and unpredictable (O’Sullivan 2018).
- Pain is the output of a highly sophisticated protective system that functions like an alarm. Potential threats to the body are detected in the periphery, and then communicated to the brain. The brain interprets the meaning of the information and creates pain if it perceives the need for protection. The sensitivity of this system can change based on many different factors, including injury, inflammation, emotions, stress, memories, and general health (Melzack 2010).
- Because pain depends on perception, tissue damage does not always cause pain, and pain can be felt in the absence of tissue damage. For example, people without pain frequently show significant damage on MRI, and back pain usually cannot be linked to any specific pathology (Brinjikji 2015).
- The link between pain, posture and allegedly defective movement patterns has been overemphasized. Research shows poor correlations, and often no correlation, between these factors (Lederman 2011). Further, pain treatment focused on correcting specific “dysfunctions” rarely outperforms general exercise (See, e.g. Foster 2018; O’Sullivan 2016; Riley 2018; Smith 2014; Ferreira 2007).
- On the other hand, psychosocial factors have been underemphasized. For example, anxiety, catastrophisizing, and fear of movement increase the risk for chronic pan, while optimism and self-efficacy predict recovery from injury (Marcuzzi 2016). Part of the purpose of providing education to patients is to favorably alter these variables (Louw 2016).
I can assure you that pain science educators do not teach that pain is in your head, that tissue damage doesn’t matter for pain, and that movement doesn’t matter for injury. In fact, I have frequently stated the precise opposite on many occasions. Here are just a few of examples, all of which date back several years. From a blog post on the poor link between posture and pain.
Don’t misinterpret the research on posture to mean that biomechanics and good form don’t matter at all. Vigorous exercise is different than just sitting or standing around, and it may require more attention to proper alignment. . . .So your posture and alignment matters in a heavy deadlift. It matters when you land a jump. It matters when you sprint, lift weights, or engage in any activity involving a great deal of mechanical stress. In these cases, it is a good idea to use conscious effort or coaching to ensure that your biomechanics and spinal alignment are optimized to distribute stress, reduce risk of injury and increase performance.
Here’s a line from book my A Guide to Better Movement, discussing the role of the brain in creating pain.
Here is a very important point of clarification: none of this means that pain is not real, or that it is all in your head. Pain is real. Pain is a real feeling, but that feeling does not necessarily reflect real damage in the body. Further, although pain depends on brain activity for its existence, this does not mean you can simply think pain away or that pain is your fault. Unfortunately, the processes which create pain are mostly unconscious and outside your control. Although your conscious thoughts about pain can change it, the effects are in many cases small.
From a blog post on pain science confusion:
pain is of course related to conditions in the body. It is just not determined by them. Even though pain requires brain activity, it remains true that in many circumstances, tissue damage will almost certainly cause that brain activity. Thus, we would all prefer to have less tissue damage than more.
Here’s Greg Lehman making the same point in his (highly recommended) workbook:
Its not all in your head! Even health professionals get this confused. As soon as people start talking about emotions, psychological factors or the brain, the assumption often slips in that we are saying your pain is now just in your head. Just because psychological factors or the brain is involved does not mean the body is not important or the pain is imagined.
Another source of nuanced information on the practical implications of pain science is Jason Silvernail, a doctor of physical therapy and strength and conditioning coach. Here is an informative interview he did with Bret Contreras.
2. MRI Research shows clearly that tissue damage without pain is common and normal
Extensive research shows that almost no matter where you point an MRI on a person over twenty, you have a very strong chance of finding significant damage, even in places without pain. Here’s an excellent infographic from Jørgen Jevne summarizing part of the evidence.
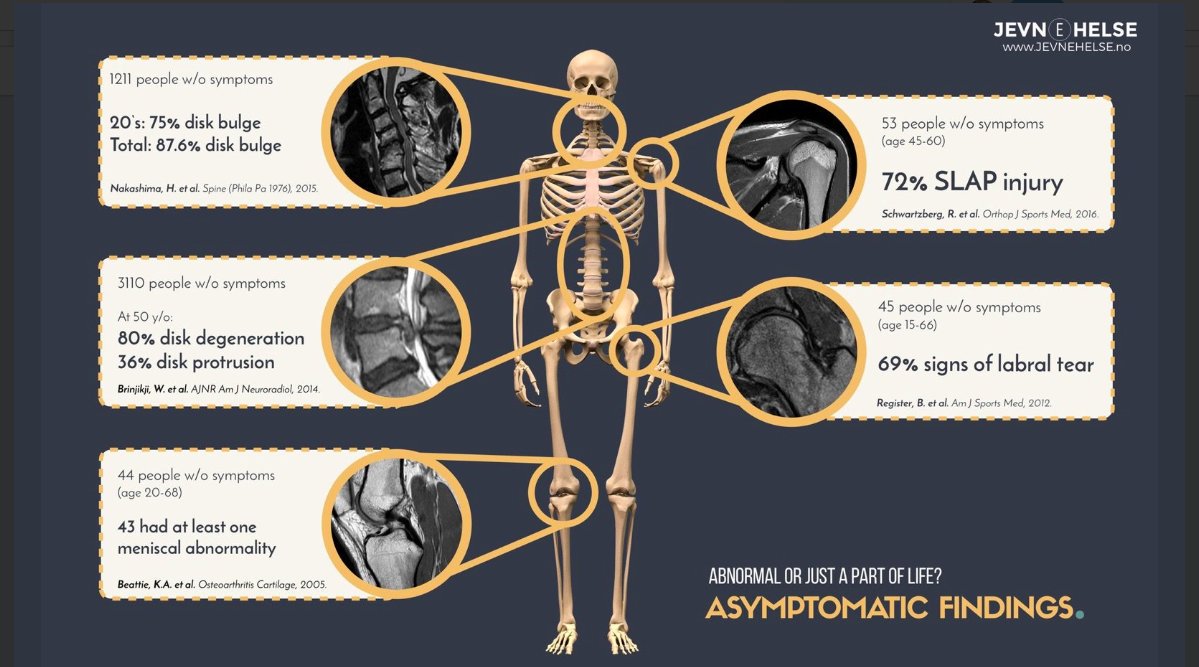
For more research see my blog post here.
This research does not mean that damage is not linked to pain. Higher levels of damage are indeed correlated with more pain, but it remains interesting that the correlation is far less than we might imagine (Brinjikji 2015). Greg Lehman provides a useful analogy – damage in the spine or other joints is like kindling for a fire that may or may not be lit by other factors.
Seedman argues that the people in these studies aren’t hurting right now, but will surely have pain in the future. But several studies have already addressed this concern. A seven-year follow up study found no correlation between initial MRIs and future pain (Borenstein 2001). Another study did a ten-year follow up, looking at the extent of disc degeneration, spondylolisthesis, disc bulge and other findings. The conclusion: “our data suggest that baseline MRI findings cannot predict future low back pain.” (Tonosu 2017). A study on shoulders of pain free overhead athletes found that forty percent had rotator cuff tears, and none had pain five years after the study (Conor 2003). Seedman cites one study to support his claims, showing that MRI evidence of stenosis predicts future back pain. But the same study also showed that many other positive MRI findings did not predict future pain, and concluded that “No consistent associations between MRI findings and future outcomes were identified.” (Hill 2018).
3. Posture has been overemphasized as a contributing factor for pain
There is a large body of research that looks for correlations between pain and measurements of postural alignment. Most find none. Here is an excerpt from my recent book Playing With Movement that summarizes some research from more than thirty years of studies:
- No association between leg length inequality and back pain (Grundy 1984).
- No difference in lumbar lordosis or leg length inequality in 321 males with either severe, moderate or no back pain (Pope 1985).
- No association between neck pain and neck curvature in 107 people over the age of 45 (Grob 2007).
- No significant difference in lumbar curve, pelvic tilt, leg length discrepancy, and the length of abdominal, hamstring, and iliopsoas muscles in 600 people with and without back pain (Nourbaksh 2002).
- Teenagers with postural asymmetry, excessive thoracic curve and/or lumbar curve were no more likely to develop back pain in adulthood than peers with “better” posture (Dieck 1985).
- Pregnant women with larger increases in low back curve during pregnancy were no more likely to develop back pain (Franklin 1998).
- A review of ten studies found no correlation between thoracic kyphosis and shoulder pain. (But there was less shoulder ROM) (Barrett 2016).
- Teenagers with slumped forward head postures didn’t have more neck pain (although they were more depressed.) (Richards 2016).
- No association between low back pain and spondylolisthesis (a condition where a vertebra has slipped forward, and which is often corrected by fusion surgery (Andrade 2015).
- In a group of women aged 65-91, those with substantial kyphosis had no more back pain or disability (Ettinger 1994).
- No association between neck pain and “text neck” as assessed by physical therapists (Damasceno 2018).
- Ergonomic programs do not reduce the risk of a future onset of neck pain, but exercise reduces the risk by half (Campos 2018).
Although some studies have found a positive association between measurements of spinal alignment and pain, these are exceptions to the rule, and the correlations are relatively weak. (Chaelat-Velayer 2011; Smith 2008). The weight of the evidence is perhaps best represented by a systematic review done in 2008, that analyzed more than fifty-four studies on the link between pain and posture. Together they did not produce evidence supporting an association between measurements of sagittal spinal alignment and pain (Christensen 2008). Although back pain is associated with scoliosis, this condition refers to relatively large lateral asymmetries that are not present in 98% of the population. (Theroux 2015).
Other relevant studies examine the effects of jobs that involve repetitive use of postures thought to be awkward or stressful. These have found that:
- Sitting at work is not associated with low back pain (Hartvigsen 2010).
- A systematic review of 35 studies found that occupations that require lifting weights probably do not cause low back pain (Wai 2010).
- A systematic review of 99 studies found no good evidence of a causal connection between back pain and occupations that involve awkward postures, lifting, bending and twisting (Kwon 2011).
- Although occupations that routinely require heavy lifting are associated with increased risk for back pain, the effect size is modest (Waddell 2001).
The above research indicates that if any correlation exists between posture and pain, it is weak. Further, even if a correlation between pain and posture does exist, this would not prove a causal relationship. It may be that pain causes bad posture, or that some unknown factor causes both. This is highly plausible. People who are injected with a solution causing back pain will spontaneously adopt different postural strategies to reduce discomfort (Hodges 2003). Yet another unproven leap is that posture can be corrected, and that the corrections serve to reduce pain.
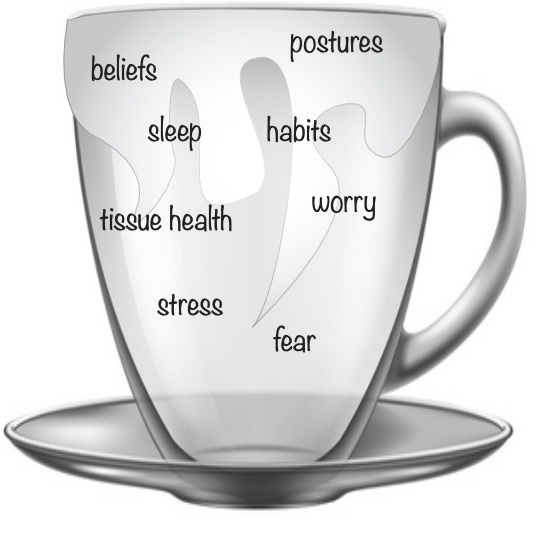
Does this mean posture never matters for pain? No, and most pain science educators will ready admit this. For example, here’s a diagram from Greg Lehman’s workbook, showing the different factors we might hope to modify to help with pain. Note that posture is one of them. But importantly, only one of many.
4. Biomechanics are complex and not easy to “correct.”
Pain science does not overrule the basic laws of physics, and therefore it is obvious that moving with bad technique under heavy load can cause serious injury. But the question remains whether we are likely to get chronic pain from everyday habitual movement patterns in low load activities like sitting, standing, breathing, bending or reaching. Do these cause repetitive stress and injury, or do we simply adapt to handle the stresses we encounter regularly, just as we do with exercise stress?
This is best answered by looking at a substantial body of research that is similar to the research on posture discussed above. It shows:
- Movement patterns that are commonly alleged to be dysfunctional are not correlated with pain or increased injury risk;
- Treatments aimed at correcting specific dysfunctions often work no better than general exercise; and
- Corrective methods may create good results even when no “correction” occurs, suggesting these methods work by some other mechanism.
For example, general exercise works just as well as stabilization or motor control exercise for low back pain. (Smith 2014; Ferreira 2007; Saragiotto 2016.) This is true even when the treatment involves an attempt to correct a specifically diagnosed movement “impairment.” (Riley 2018, Dillen 2016, Azevedo 2018).
There is a similar pattern for shoulders. General stretching and strengthening works just as well as motor control exercise to correct scapular “dyskinesia.” Further, people improve on motor control programs even when movement patterns stay the same, suggesting the active ingredient is simply exercise, and not correction of any defect in coordination (See Camargo 2015, McClure 2005, Timmons 2012, Ratcliffe 2014, Struyf 2013). For example, Struyf 2013 concludes that most scapular movement patterns alleged to be dysfunctional probably represent “normal movement variability.”
For knee pain, it seems that the most effective treatment is simply strengthening the muscles around the hip and knee, even when this is done through allegedly “non-functional” exercises with knee extension machines (Willy 2016, Rabelo 2018).
Although Seedman talks at length about the importance of correcting defective movement patterns, he does not specify any such patterns in his article, or how to assess and correct them. He makes vague reference to the importance of strong glutes and core muscles for back pain, but does not cite any studies on this issue. In fact, core strengthening works no better on average than general exercise for back pain (Lederman). Further, the idea that inactive glutes cause pain is not well-supported by research, which has often shown that pain is associated with more glute activity not less (Kim 2014, Lehman 2006, Suehiro 2015, Dwyer 2013).
The lesson here is that the connection between movement and pain is complex. There’s no doubt that exercise can reduce pain, improve function and help to prevent injury. But we should be very skeptical about claims concerning the assessment and correction of ”dysfunctions” and their relevance for pain in everyday movements (Tuminello 2017).
5. Inflammation
Seedman suggests that pain scientists ignore the role of inflammation in pain. I have no idea what he might mean here. The role of inflammation in sensitizing nociceptors is one the most basic facts about pain physiology, and also illustrates a key principle of pain education – pain sensitivity can change even as tissue damage stays constant.
Seedman notes that high levels of chronic inflammation are associated with bad health, pain, and reduced function in gait pattern, walking speed, strength, stability, and mobility. This is in no way surprising. If someone is in poor health and has high levels of inflammation, we would expect that they won’t be moving well or feeling well. Seedman’s evidence demonstrates this obvious connection, but it doesn’t show that the inflammation is caused by poor posture or movement patterns. If it was, then research would easily find correlations between posture and pain, but it doesn’t.
Conclusion: The Truth About Pain Matters
I think getting this information right is incredibly important. Chronic pain is one of the biggest health problems in the world. We have no magic bullets to cure it, but the best hope for progress lies with understanding it better through science, and getting people moving. Personal trainers are in an excellent position to do both. There is still much we don’t know, and healthy criticism is needed to move the ball forward. But we know enough to take action – there is a huge gap between common practice and well-established evidence, and that needs to be closed.
Thanks for reading this far! Please share this article with anyone who has questions about pain science. Or point out mistakes if you see them. Please also remember that debate is far more productive when it is respectful and polite.
This was originally posted on Todd Hargrove’s website. You can click here to read more blogs from them.
Want to learn more from Todd Hargrove?
He has done a Masterclass lecture series for us on:
“Pain, movement and play: common sense for complex problems”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Great article Todd, yes many people are arguing about what others are saying but unfortunately ego and frustration may be clouding the perspective of the article or what the people may be trying to say. Thanks for a great overview of not only the research but also your own experience. OD