
Anterior knee pain is super common – understandably, we tend to think of the patellofemoral joint, Hoffa’s fat pad or proximal patella tendon as the main culprits. For an in-depth look at assessing and managing patellofemoral pain in particular, check out this Masterclass by Claire Patella.
However, there are other less common causes that might not necessarily be on your clinical radar but are certainly important to consider. This blog aims to shed some light on other conditions to help with your differential diagnoses.
Quadriceps insertional calcific tendinopathy
This has a similar symptom provocation pattern to patella tendinopathy. When pain spreads it can even mimic patellofemoral pain (PFP). This includes jumping sports but also powerlifting, martial arts and bodybuilding (question anabolic support). Incidental calcific changes are found very commonly in active populations (e.g. cyclists).
Exam:
- Presents with pain on a deep squat and hopping.
- Focal suprapatellar tenderness and you may need to examine in variable degrees of knee flexion; or compress distal patella to elevate proximal pole and expose irritable tendon zone for palpation.
- If the condition evolves, it may have diffuse pain in the suprapatellar pouch potentially due to concurrent quadriceps fat pad inflammation.

Figure 1
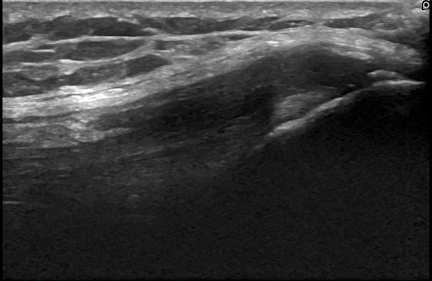
Figure 2
Patella stress fracture
Traumatic patella fractures are well recognised. However, stress injuries can potentially occur (although rarely) in those with poor bone health, low bone mineral density (e.g. RED-S), and in patients struggling during rehab post patellofemoral surgery with profound extensor mechanism deconditioning.
In figure 3 below, the distal pole stress injury has progressed and completed to full fracture of the distal pole with a cortical breach. This occurred when simply stepping off a curb with several weeks of preceding pain.
Exam:
- Can present with ‘sympathetic’ (reactive) joint effusion. Local prepatellar soft tissue swelling and focal pain due to periosteal inflammation.
- These patients will likely be unable to single leg squat or hop and may be ‘shut down’ functionally (e.g struggling with stairs). Assess for any ‘extensor lag’ if very painful (e.g. on SLR and against resistance).
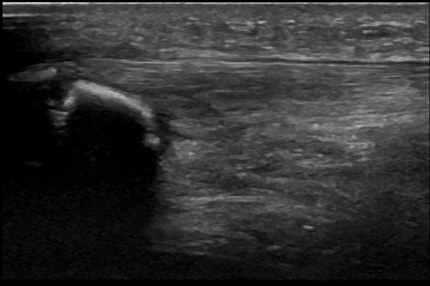
Figure 3

Figure 4
Trochlear groove pathology
This is likely one of the more common pathologies on this list but it is under-appreciated that ultrasound can evaluate joint surfaces – knee hyperflexion exposes a significant portion of the groove. It can assess for osteoarthritis, osteochondral defects and morphology.
Figure 5 below shows one patient who has a shallow dysplastic trochlear. Figure 6 is another with extensive chondropathic changes. It can also pick up chondrocalcinosis (figure 7) which commonly affects the patellofemoral joint cartilage – a phenomenon seen in pseudogout and haemochromatosis.
Exam:
- This presents as variable, diffuse retro or suprapatellar pain with effusion.
- Pain with patellofemoral compression, glide and Clarke’s test (although be mindful that this is sore for many people, even those without pathology).
- (Osteo)chondral defect – predictable catching pain at specific knee flexion angle and shift to contralateral side on squat.
- Occasionally palpable tenderness in groove with knee in flexion, or in parapatellar pouches.
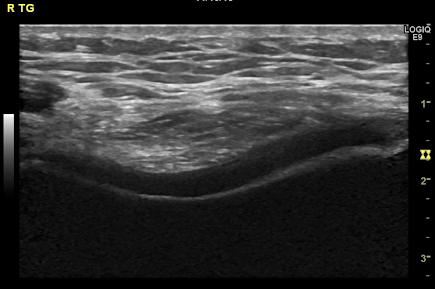
Figure 5
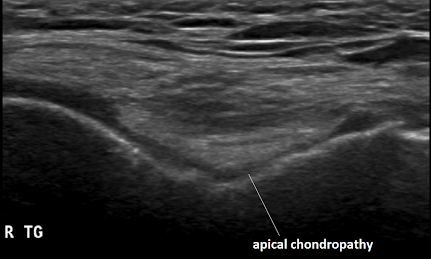
Figure 6
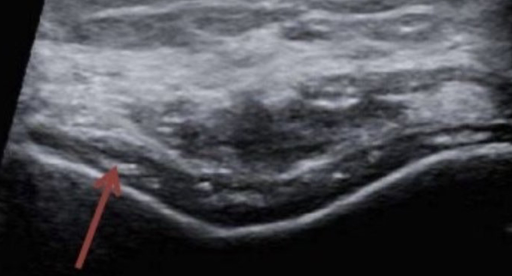
Figure 7
Retinaculae
We tend to overlook these, but pathological changes & thickening can hint at wider pathology (e.g. chronic patellofemoral instability).
Medial patellofemoral ligament (MPFL) integrity can be assessed in the acute patellofemoral dislocation setting.
Very occasionally they can generate pain under loading (e.g in this lateral retinaculum calcific case, figure 8).
Exam:
- Atypical focal tenderness at medial or lateral patella border; there might be ‘bony’ palpable thickening (calcification).
- Pain on functional patellofemoral joint loading localising to the retinaculum.
- May well have coexisting patellofemoral joint pain signs and symptoms of chronic instability / subluxation episodes or previous traumatic dislocation (e.g. OCD).
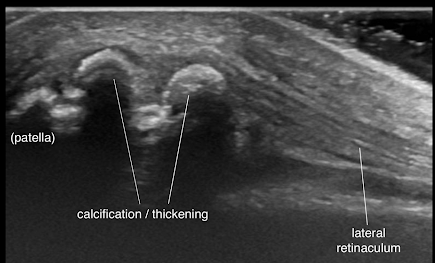
Figure 8
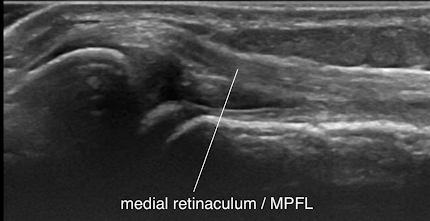
Figure 9
Bipartite patella
A patella with an unfused ossification centre, most commonly found superolaterally.
These are typically asymptomatic and usually an incidental finding on imaging, but 2% can cause symptoms.
The synchondrosis (‘joint’) between the main patella and ossicle can become inflamed, triggered by overload (e.g. jumping or high impact sport) or direct trauma to the patella (making the ossicle unstable).
Some consider excessive vastus lateralis traction to be implicated.
The bipartite morphology can easily be picked up on US and x-ray – but may be confused for a patella fracture.
The MRI images (figure 10 and 11) show bony oedema in the fragment and around the synchondrosis which suggests it is symptomatic.
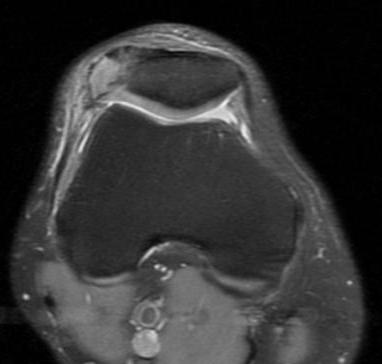
Figure 10 (Kavanagh et al., 2007)
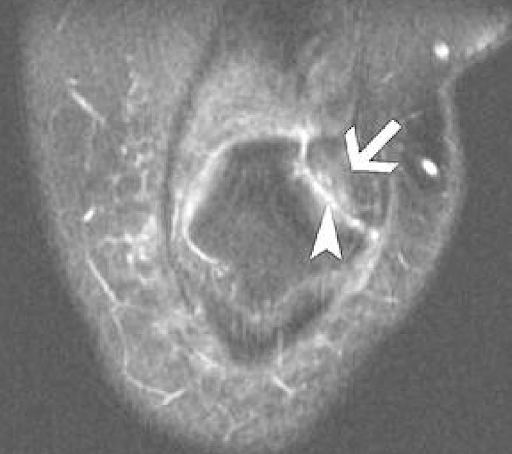
Figure 11 (Kavanagh et al., 2007)
Exam:
- Clinical signs may overlap considerably with patella stress fracture and retinaculae as detailed above.
- Pain on squat, hop, jump – reduced power output.
- Tenderness at superolateral pole; possible focal swelling.
Fat pad injury
Assessment of Hoffa’s fat pad inflammation is unreliable on ultrasound vs MRI (some clinicians disagree).
But trauma causing contusion and scarring to the fat pad can be picked up – this case (figure 12) resulted from a heavy blow in a direct ‘front on’ rugby tackle to the anterior knee.
Quadriceps fat pad and Hoffa’s impingement can also be identified on dynamic knee ultrasound assessment.
Exam:
- Positive ‘fat pad compression test’ – infrapatellar squeeze and passive knee extension.
- Pain on passive knee hyperextension.
- Familiar, reproducible (painful) ‘click’ on active knee ROM.
- Focal pain and palpable thickening on palpation into traumatic impact area.
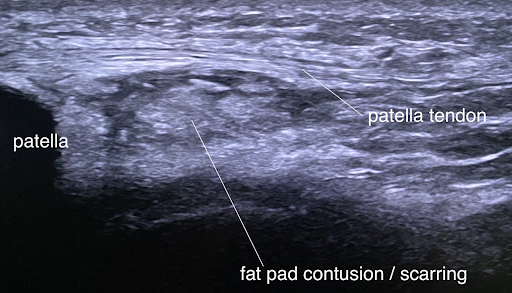
Figure 12
Bursitis
Easy to pick up on ultrasound both prepatellar and deep – In figure 13, we see a huge prepatellar bursitis – hypo / anechoic swelling, sometimes with synovial fronds or bodies seen.
With smaller superficial bursae, we have to be gentle with probe pressure otherwise they disappear under compression.
Repetitive compression, friction and direct blow trauma is usually the mechanism but beware an underlying rheumatological driver.
Exercise caution with putting needles in due to the risk of infection. Try and manage conservatively if possible.
Exam:
- Prepatellar bursitis – tender, fluctuant, warm superficial swelling – try and distinguish it clinically from an effusion.
- Deep infrapatellar bursitis are better at hiding and to identify clinically – tenderness just proximal to tibial tuberosity and focal swelling deep to patella tendon if large.
- Perceived limited knee flexion due to ‘tightness’ – but often objectively patient has reasonable ROM with encouragement or distraction.
- Look for signs of local infection such as cellulitis, wound, puncture skin breach.
- If no clear overload or traumatic cause – scrutinise joint and explore history for other inflammatory causes, (e.g. RA, gout etc).
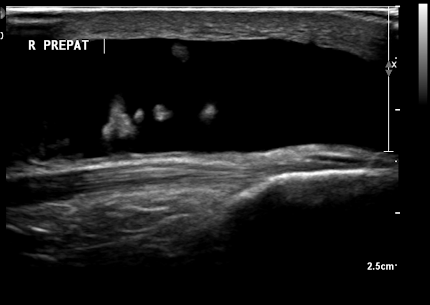
Figure 13
Patellar tendon enthesopathy
Distal or insertional patellar tendinopathy is far less common than proximal.
In figure 15, we see a classic enthesopathic presentation with cortical and bursal changes at tibial tuberosity in a patient with ankylosing spondylitis.
In ‘at risk’ rheumatological groups, be mindful of an inflammatory cause of insertional patellar tendon pain.
Patients may have unilateral or bilateral knee symptoms and find NSAIDs modify pain significantly and are reliant on them for a better quality of life. Resistant to traditional ‘loading programme’ approach for tendinopathy.
Can happen in adolescents as well (e.g. enthesitis related juvenile arthritis) – so have at the back of your mind that not ALL tibial tuberosity pain in this group is Osgood-Schlatters disease. Figure 14 below is an excellent tool developed by Paul Kirwan to help identify those with spondyloarthropathy.
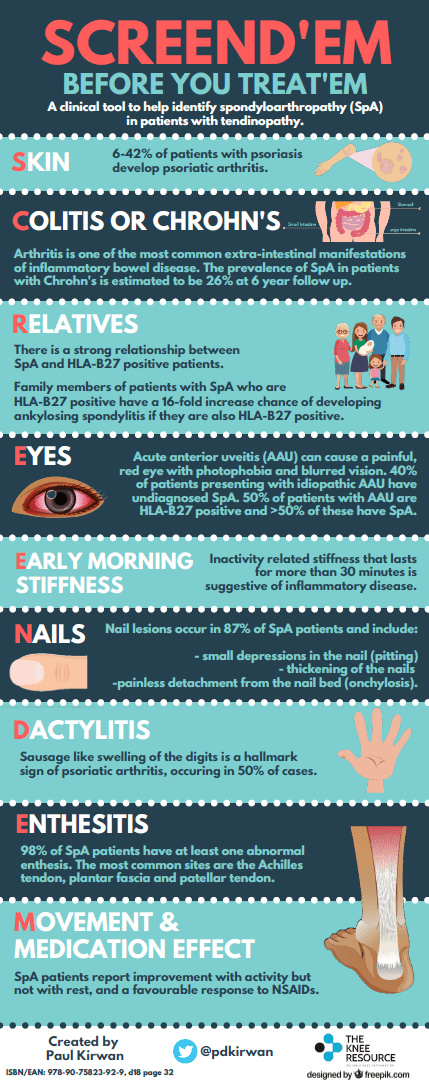
Figure 14 (Kirwan, 2019)
Exam:
- Tibial tuberosity tenderness and local soft tissue swelling around tendon and infrapatellar bursa is suspicious.
- Concurrent knee joint effusion and synovitis.
- Screen other small joints and entheses (e.g. achilles and plantar fascia) – look for axial / SI joint signs, including reproducible gluteal pain.
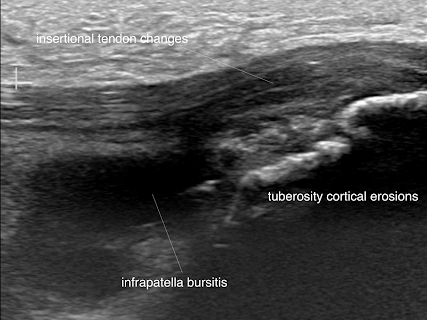
Figure 15
Parameniscal cyst
Most commonly seen at lateral joint line – but in figures 16 and 17 we see a huge multi-separated cyst buried in Hoffa’s fat pad derived from an anterior horn lateral meniscal tear.
In this case the cyst had almost completely disappeared – or maybe decompressed? – when brought back a few weeks later for US guided aspiration.
The patient may describe uncomfortable loss of extension clinically masquerading as fat pad impingement, but may also have other more ‘classical’ mechanical meniscal symptoms.
This potentially needs MRI to assess underlying meniscus pathology.
Exam:
- Effusion related to the meniscal tear (unlikely in fat pad impingement).
- Uncomfortable ‘fullness’ or swelling in medial or lateral infra-patella pouch, assessed with knee in partial flexion.
- Painful spongy block to terminal passive knee extension.
- If your battery of meniscal tests are positive, this increases sensitivity for a tear.
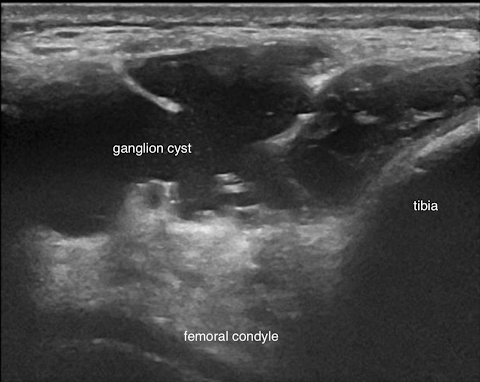
Figure 16
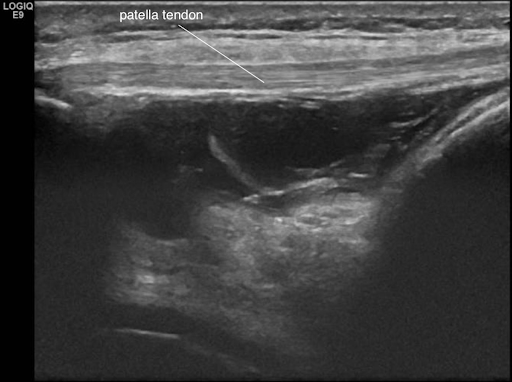
Figure 17
Medial plica
Often considered a ‘dustbin diagnosis’; partly because historically it’s been blamed too frequently for retropatellar or medial parapatellar pain before assessing and ruling out far more common causes – but admittedly – they can occasionally become inflamed and symptomatic.
Figure 18 demonstrates a thickened plica visible on ultrasound.
The confirmed cases I’ve seen have mainly been in cyclists.
The patient may describe predictable painful catching or clicking particularly when the extensor mechanism is under load through active flexion.
Consider in cases of what appears to be recalcitrant ‘PFP’.
Exam:
- Mild, grumbling effusion.
- Tenderness or palpable thickened band in medial parapatellar pouch.
- Uncomfortable catch and click felt medial to patella on squat or at a consistent knee flexion angle on taking joint through passive range.
- Passive medial patella glide is usually provocative.
- Positive Stutter test.
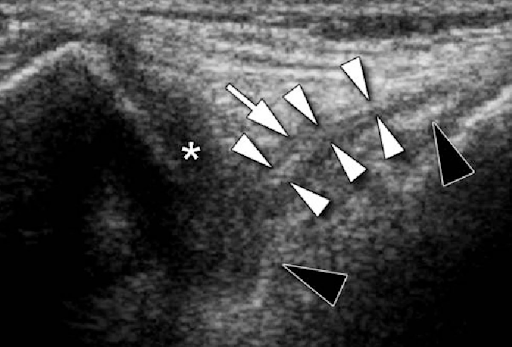
Figure 18 (Paczesny & Kruczynski, 2009)
Wrapping-Up
This blog outlined uncommon causes of AKP. Although some of these conditions are rare, I hope you found it informative and clinically useful. If you want to learn more about assessing and managing anterior knee pain, check out Claire Patella’s Masterclass on Patellofemoral Pain.
Want to learn more about anterior knee pain?
Claire Patella has done a Masterclass lecture series for us on:
“Patellofemoral pain”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!