
I love this area, but it can be confusing and seemingly complex – especially as there is significant overlap between groin pathologies along with clinical behaviour and presentation. Not to mention the concurrent pain drivers ‘muddying the waters’ further. This blog will skim the surface. So if you want more detailed information, check out Dr. Andrea Mosler’s masterclass on Groin pain in athletes: unraveling the mystery.
1. FADDIR test (Flexion Adduction Internal Rotation)
This is my ‘go-to’ test alongside the ‘hop’ and should be the first test done in supine.
If this is negative, then it’s unlikely the joint is driving the pain (e.g. Femoral acetabular impingement, labral tear, OA, avascular necrosis).
However, you can have a positive FADDIR with proximal femur stress fracture. So remain vigilant!

Figure 1. FADDIR test (DiSilvestro et al., 2013)
2. ‘The Hop Test’ – ipsilateral
This is not a specific test but sensitive for pelvic and femoral bone stress injuries.
Patients will be ‘shut down’ (not bouncy!) and leaden-footed.
If it’s negative, then you can be comfortable knowing it’s not a high grade stress fracture.
Below is an example of this, an elite runner in his 20s. He presented with a 6 week history of left groin pain travelling to the thigh along with night pain and symptoms worsening on warm up. He was initially treated as a hip flexor strain. The below video shows the hop test comparing right versus left. He also had a positive FADIR and ultrasound (see figure 2 below) suggested periosteal reaction of the femoral neck. Hip flexor injury in an endurance runner? Maybe think again.
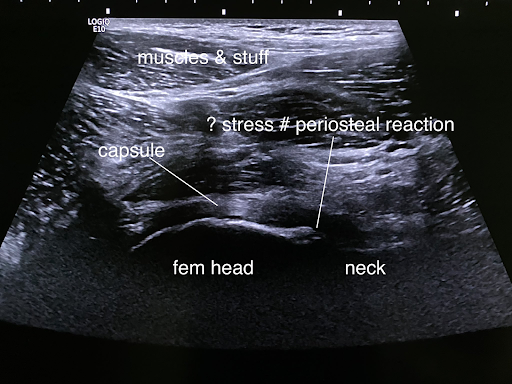
Figure 2. US image of above patient
3. ‘’The Hop Test’’ – contralateral
If the patient’s pain is triggered by hopping on the asymptomatic side, this suggests pain is generated by forces applied across the pelvis and symphysis pubis – therefore, pubic overload / stress could be a likely culprit.
It also essentially rules out other causes of ipsilateral groin pain (e.g. hip joint, hip flexor, adductor).
So it’s a rare but useful sign!
4. Reactive muscle inflammation
With pelvic stress fractures, local inflammation can occur in a muscle group adjacent to the culprit bone (e.g. adductor longus, magnus or obturator). Check out figure 3 and 4 to see this presents on ultrasound (US).
This can masquerade clinically as the ‘primary’ injury with muscle tightness / spasm and pain on resisted testing and palpation.
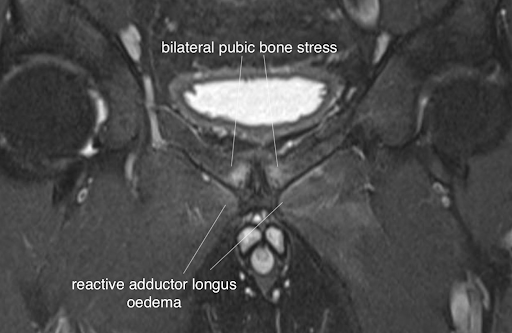
Figure 3.
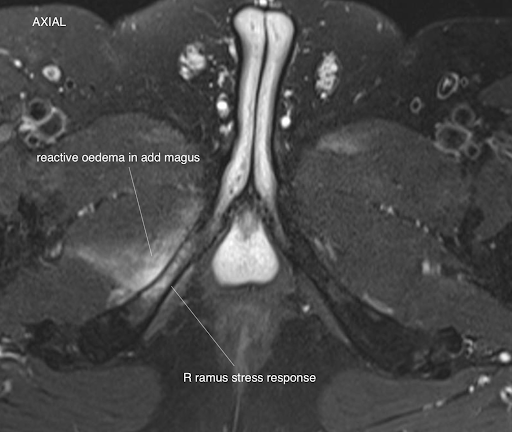
Figure 4.
5. Midline pain
If lower abdomen and groin pain randomly shifts from side to side, then invariably it’s driven from a ‘midline’ structure (e.g. symphysis pubis or pubic stress, rather than it being a bilateral injury).
A glide through the pubis usually brings on the symptoms but there are some cases where palpation is minimally provocative; rather it requires shear stress under impact or contraction load.
Although less common, the alternative is a discogenic problem (again, a ‘midline’ driver). Discogenic pain referral patterns can wrap around the pelvis into the hips and groin. Therefore, screen the lumbar spine.
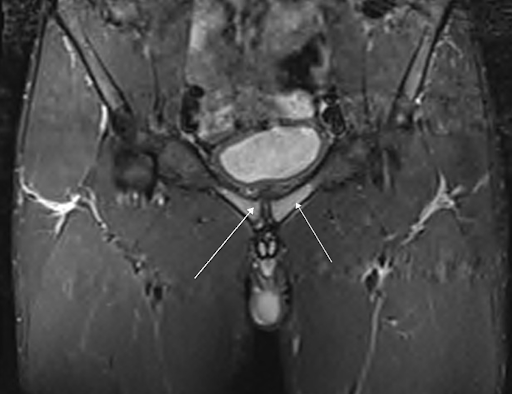
Figure 5.
6. Groin pain with genital / scrotal, perineal & perianal referral
Pain in these areas is often referred from pubic stress or symphysis overload, alongside lower abdomen pain. This is NOT typically adductor related.
If there are co-existing neuropathic features – nerve entrapment tops out on the differential diagnosis list (e.g. ilioinguinal and genitofemoral nerves). Check out figure 6 for a visual representation of nerves that could be the culprit.
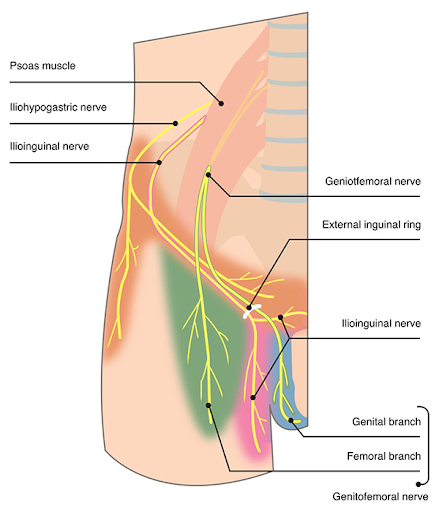
Figure 6. (Groinpainclinic.co.uk)
7. Nerve Irritation
This can co-exist with a ‘groin disruption’ pattern – scarring / inflammation in the inguinal canal. Neuromas are well recognised entities by groin surgeons.
An ultrasound guided canal block can help tease this out further alongside exercise or clinical provocation testing.
8. Inguinal related groin pain
Lower abdominal pain is key here alongside pain on cough / sneeze, core and abdominal work and a tender superficial ring on invagination (be gentle!!).
A positive ‘Cross-Over’ test is a useful sign as well.
Terms you may have heard of include ‘Sportsman’s hernia’ and ‘Gilmore’s groin’. These are old school outdated terms now and not a true hernia.
Even dynamic ultrasound and MRI don’t reliably exclude these, so exploring the mechanism of injury, pain behaviour and undertaking a comprehensive exam all become even more important.
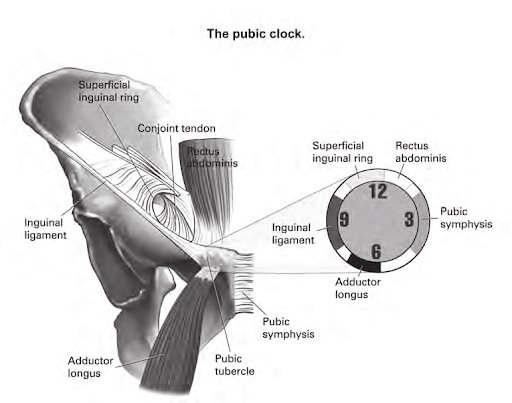
Figure 7. (Falvey, 2009)
9. Hernia
The classic ‘old man’s’ inguinal direct or indirect hernia can still exist and cause pain in the young sporty patient. Don’t miss it!
If no clear bulge or cough impulse over deep or external ring in supine, stand them up and repeat assessment – this is more sensitive with gravity assisting.

Figure 8. (Ref: Center for hernia repair)
10. Hip flexor pain
To be blunt, this is over-diagnosed! In an endurance athlete, it’s less likely to be hip flexor driven compared to a sprint, power athlete or your standard cross fitter.
Secondary hip flexor symptoms can occur due to a primary hip pathology (e.g. synovitis or dysplasia) and proximal femur stress fractures – be open minded about possibilities beyond the hip flexor pain.
Every few weeks I get a groin pain referral querying hip flexor tendinitis or bursitis. The below MRI figures show how a primary medial NOF stress fracture causes adjacent iliopsoas tendon irritation at lsr troch.
Isolated hip flexor injury is unusual so have a low index of suspicion for an underlying primary problem.
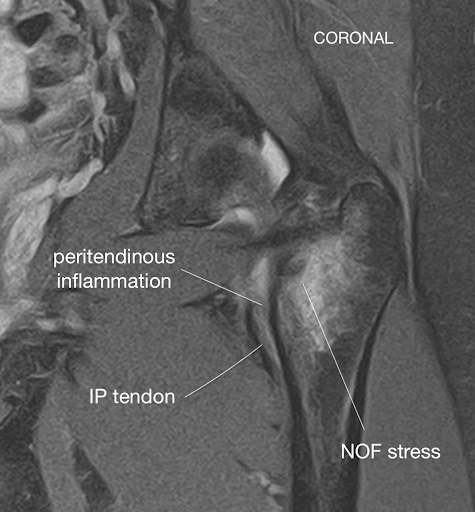
Figure 9
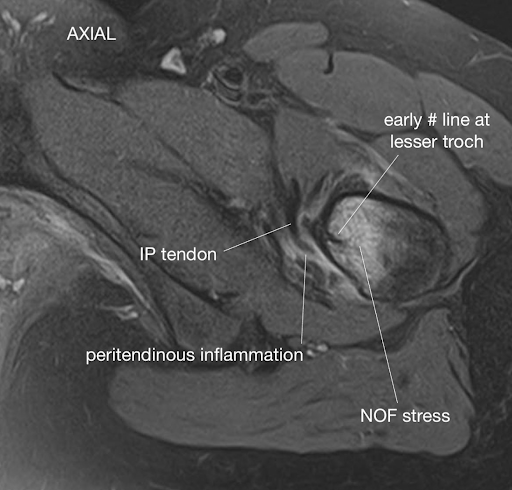
Figure 10.
11. Adductor related groin pain
This occurs in multidirectional, explosive sports (e.g. rugby, football, hockey).
Re-consider the diagnosis in runners, endurance athletes and cyclists (unless added in recent unaccustomed sprint / track sessions or S&C work).
These will have a positive squeeze test; bear in mind the adductors also act as a hip flexor, so you may have pain reproduction on resisted hip flexion especially in modified Thomas position from hip extension.

12. PLAC
Traumatic adductor injuries (e.g. avulsions) can also extend to involve the wider pyramidalis-anterior pubic ligament-adductor longus complex (PLAC).
The symptoms and clinical signs can overlap with pubic and rectus abdominis driven pain (e.g. pain on resisted hip flexion, trunk flexion / crunches (5).
Pectineus muscle injury often coexists with these (6).
13. Sacroiliac Joint (SIJ)
The SIJ can also drive groin, ramus and perineal pain – but is usually associated with gluteal pain.
Explore further in the younger demographic < 45 years old (use SCREEN’DEM as per below figure) and peri / postpartum women.
Use the Laslett SIJ test cluster as part of your objective assessment.
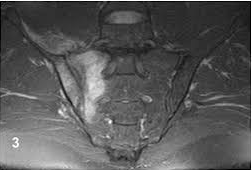
Figure 11.
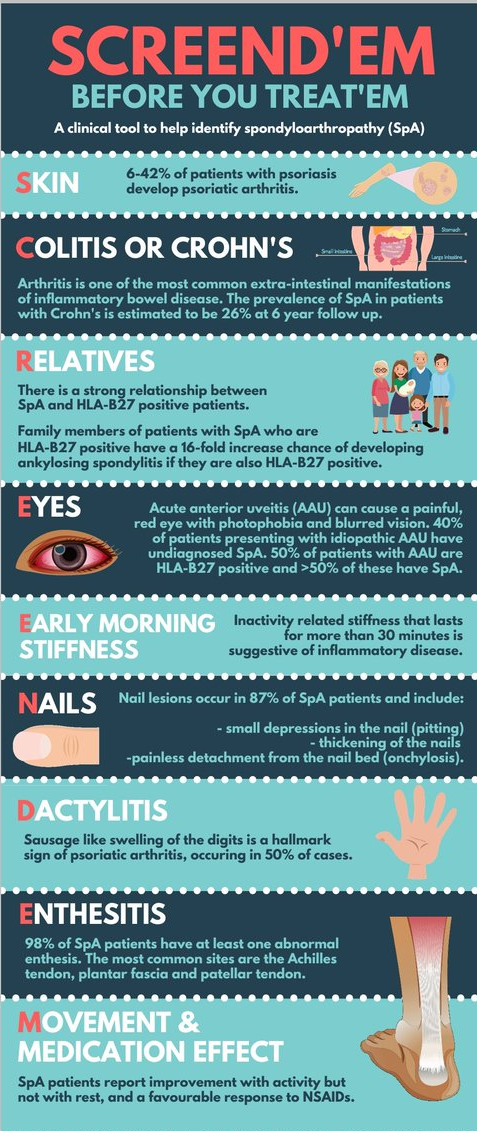
Figure 12. (Kirwan, 2019)
14. ‘Non MSK’
Remember to ask your systems questions such as – discharge, dyspareunia, bloating (gynae / pelvic); haematuria, dysuria (urinary / renal tract); diarrhoea, bleeding (GI) as well as exploring constitutional symptoms (e.g. weight loss, fever, night sweats)
Be wary of symptoms unrelated to activity / sport. Figure 13 provides a nice outline of non-msk drivers of abdominal pain.
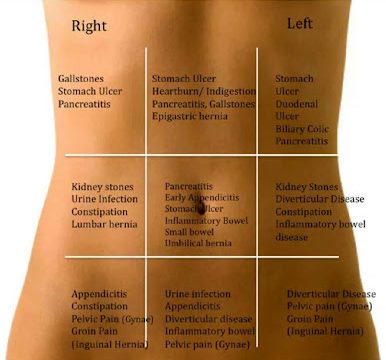
Figure 13 (Reference: Dailymotion.com)
Wrapping Up
That concludes the blog on all things groin related. If you want to learn more about groin pain in athletes, check out Dr. Andrea Mosler’s masterclass on Groin pain in athletes: unraveling the mystery. As always, thank you for reading.
Want to learn more about the groin?
Dr Andrea Mosler has done a Masterclass lecture series for us on:
“Groin pain in Athletes: unraveling the mystery”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!