Clarifying Concussion For Clinical Practice

The long term implications of concussions have been a talking point for some time now. Often it’s centred around sobering articles that show how repeated, poorly managed concussions have affected retired athletes’ lives from some of our most loved sports (1-4). Thankfully there is hope, with the ability to fully rehabilitate patients after a concussion, we can reduce the risk of these unfortunate incidents. Improving our concussion identification and management in general outpatient musculoskeletal practice will amplify the impact we can have as clinicians.
Whether you know it or not, there is already a non-trivial portion of your musculoskeletal caseload recovering from concussion; Motor vehicle (MVA’s) (34.4%), general household and leisure related accidents (53%). It is important to check for concussion in any patient we are treating after higher energy trauma or whiplash type mechanism (5). Furthermore, each year approximately 18000 people with concussion present to ED in Australia, with likely 10 x that going undiagnosed (6), with a staggering 1.3-3.8 million in the USA as a comparison (7). Therefore, I will aim to demystify the management of concussion.
All you have to do is tweak a few of your already amazing rehabilitation skills, and master a few basic new assessments to open yourself up to the possibility of helping this patient group. The best bit is that with good concussion rehabilitation, you’ll find yourself getting a bit playful and creative when it gets to dual task retraining. It really is a nice break from the daily grind of private practice physiotherapy. Sounds inviting right?
Okay. Lets Jump in!
This blog only covers the basics to get you started. For a comprehensive development of these skills I would suggest Mike Studer’s Masterclass on Concussion Assessment and Treatment (7), as well as a read of these following papers (8-12).
So what key areas do we need as a minimum to be effective?
1) Aetiology, and pathophysiology.
Concussions are a mild traumatic brain injury caused by 2 primary mechanisms. The first is a neuronal shear force, such as in the midbrain, basal ganglia, cerebellum etc. This is where our cortex accelerates on a relatively stationary midbrain. The second is the coup, contrecoup injury created from direct impact of the brain on the inside of the skull (as seen more commonly in the frontal cortex, and parietal / occipital lobes). Often a secondary ischemic penumbra can occur, which is the area around the affected brian tissue that is also damaged by the acute inflammatory response.

The pathophysiology of concussion is one of diffuse axonal depolarisation. The impact or shear injury creates this widespread depolarisation of multiple anatomically neighbouring axons, in turn leaving neural networks temporarily disrupted. This abrupt mass depolarisation leaves the brain in a large metabolic deficit, which normalises later than common symptom resolution timepoints. This partly explains why a second concussion shortly following the first is much slower to recover (7-11). Patients with concussion will present with slower conduction rates and lower cerebral blood flow, especially in the association centres of the brain, until full physiological recovery, often months post incident (7).
2) Identifying concussion
When you say concussion the common mechanism which comes to mind as a physio is standing on the sideline on a sports game and seeing a head-clash with the athlete stumbling around after. However as we now know axonal shear is also a common mechanism. For this we need to be thinking of any unexpected rapid deceleration type injury, such as a whiplash. The common symptoms we need to be looking out for are covered in the SCAT5 assessment tool attached here (13,14).
Knowing there are subtypes of concussion is also useful, as it allows you to know what type of activity may bring on the symptoms, and where you should focus your rehab. The following table outlines a nice pneumonic to remember these.
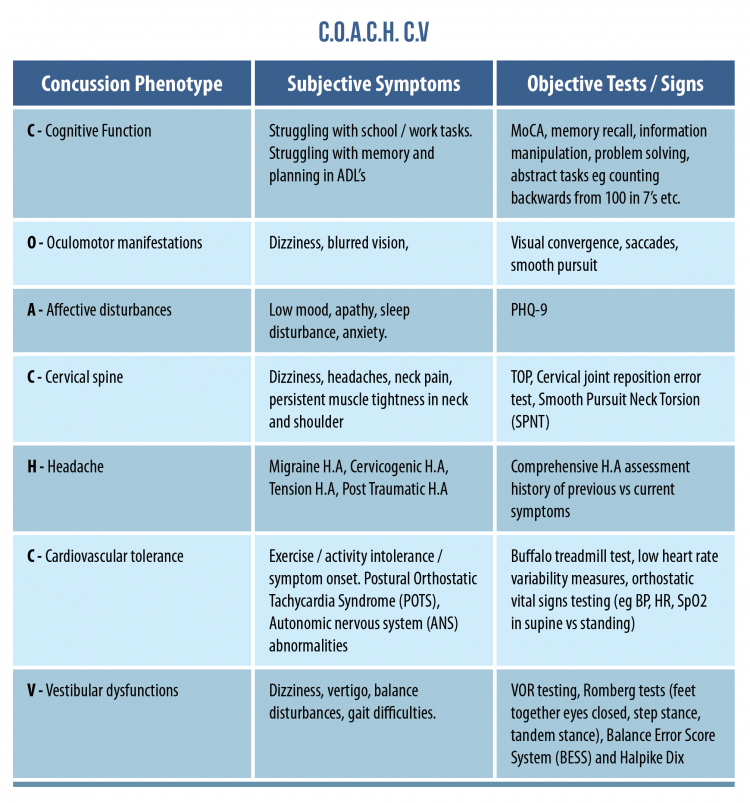
Don’t make the mistake of thinking you need to test all of this, or that you need to get it right first time, just listen to your patient’s story and let their subjective experience guide your clinical reasoning.
3) Prognosis
After a first concussion, a second is 1.5 x more likely to occur, and a third approximately another 3 x more likely again. Luckily most concussions go on to spontaneously resolve within 14 days in adults >18 years old, or 4 weeks <18 years old, with only between 10-30% progressing to prolonged concussive syndrome (PCR). PCR is described as still having concussion signs and symptoms >3 months post the initial injury (6-11).
But it’s not only about the brain!
The risk of lower limb injury in the year post concussion seems to be appreciably higher (15,16). This risk gets linearly higher again with each subsequent concussion that an athlete receives (15). This is likely due to the many factors that the brain plays in the dual tasking aspects of our life, and how these, unlike the overt symptoms, don’t spontaneously resolve (6,15-17). So if we want to minimise the risk of harm, while maximising the possibility of performance, full rehabilitation is a must.

4) Treatment
Finally, how do we go about making sure our patients fully rehabilitate and reduce the risk of a second concussion, or a season ending lower limb injury?
Well it seems there are a few key things we can guide to facilitate successful rehabilitation.
- Moderate intensity exercise, 20 mins 1-2 times per day, or;
- 80-90% of symptom limited HR threshold (for cardiovascular phenotype) obtained from the buffalo treadmill test (18-21).
- Follow your sport specific graded return to play protocols: examples in the references (22-24).
- Dual task retraining: This one requires slightly more assessment to get the right dose for prescription.
The idea of dual tasking is that the brain is able to cope with the load of a cognitive task and a motor task at the same time without any decrements in performance on either. Any decriments are called a “Dual Task Cost”, and can be an outcome measure for progress (7-17).
The rehab continuum for motor tasks is as follows in order of early / late stage rehab:
- Balance (e.g. romberg’s test).
- Gait (TUG, 10m Walk test, 40 yard dash).
- Work / sport specific (e.g. keystrokes / minute typing, free-throw % accuracy)
After getting a baseline for performance on any of the above you also need to get a baseline of performance in a cognitive information processing task from the list below. Choose what’s most appropriate for your patient:
- Hold / short term memory (recalling just learnt number sequence, words, names, skills).
- Process / Manipulate (given information and having to come up with the best solution).
- Generate (Having to come up with as many bits of relevant information to a topic stimulus as possible, e.g. name all the tasks you do in your sport).
- Recall / long term memory (ability to recall known relevant historical facts / figures)
Then we add them together and assess the dual task cost:
((single task – dual task) / single task))*100%
The final step is to turn this into a fun exercise to do in the clinic and at home. This means the physio can bring out their creative side at every step of rehab and really immerse themselves in individualising the process as well.
Example 1 – Your patient plays rugby? Sweet, let’s grab a ball, go to the park, and have them pass a ball at a target while naming all the players in their team.
Example 2 – An injured electrician on workers compensation, let’s set up a mini step ladder holding something above their head and doing mental arithmetic.
Repeat these exercises while you continue to assess the dual task cost. When there no longer is any, it’s time to upgrade. Rehabilitation can only be considered complete when they have progressed to performing their goal task within the goal environmental context, with no dual task cost. Then the patient is ready to return to their sport / work with no restrictions (7).
Wrapping up
So there you have it. Hopefully this blog has clarified concussion for your clinical practice and lit the spark for you to get out there and help this often undertreated patient population. For more depth on this topic check out Mike Studer’s Masterclass on Concussion Assessment and Treatment.
Want to become a pro at managing concussions?
Mike Studer has done a Masterclass lecture series for us on:
“Concussion: Assessment and Treatment”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!