
In this blog I will aim to outline a pragmatic and in-depth approach to rehab programming in active populations. My hope is that this will act as a guide for physiotherapists and other rehab professionals to direct clinical reasoning throughout the rehab journey. I will outline what we need to see in each phase of rehab to ensure we can accurately assess functional capacity and mitigate risk to the patient while they are still training. This will also allow us to communicate the important things that stakeholders (athlete, coach, S&C) actually want / need to know or do. For a more thorough look at the S&C coaches perspective on rehab, see here (1).
I believe the physiotherapy model actually outperforms the traditional S&C model in its approach to clinical reasoning in rehab. Physiotherapy uses a session to session approach, with constant assessments to dictate exercise prescription (bottom up approach). S&C commonly use a periodisation approach (top down approach). Top down approaches break training into set blocks of time that progressively build into the next set block (2). Doing things the more “physio way” with rehab allows you to adjust your programming on a session by session basis along the continuum I will outline below. This can help avoid situations of conflict with stakeholders, when things don’t go exactly to a pre-planned program.
This continuum has been developed very much in line with the principles from Sam Blanchard’s Masterclass (3) as well as the best available evidence on return to sport phases and protocols (4,5,6,7,8,9,10,11). It follows the basic premise of 4 questions in any phase:
1 – What is the capacity of the tissue now?
2 – How can I improve capacity now?
3 – What tolerance levels / physical capacities does the patient have to demonstrate to progress?
4 – What is the final capacity the patient needs?
Note – Not every patient needs to start at phase 1 (“Early acute”) in the continuum below, and finish at phase 5 (“Performance”). Just find where they are currently and where they need to go. Note – progression through these phases should always consider the patient’s psychological and social factors pertaining to rehabilitation progression.
Ok, let’s rip into it!
Early/Acute and Early > Mid Phase

These initial two phases are Physiotherapy 101: Initial management, symptom modification / monitoring, and finding an entry point to loading (eg PRICE, POLICE, PEACE and LOVE if acute). Often we are having to progress through ROM limitations, tissue tolerance to stretch (be it passive, active or active assisted), and doing some form of ‘muscle activation / control’ work. Common constraints here are pain, irritability, fear avoidance and volume load tolerance limitations. Somewhere in these phases things begin to settle and we can start to make the most of the principles I spoke of in my last blog (14) to aid in the remodelling of tissue. These phases end when we can prove tolerance to higher volumes of low external load work (think 3 sets a couple of times a day of “go till it burns” theraband, or low level “control” exercises). Most physios are very comfortable taking this phase.
Essential communication to stakeholders
- We can see you/they are tolerating some loading now.
- Tissues are starting to positively adapt and will be ready for more effective training soon.
- Give solutions to continue to train other body parts / systems around the injury and how to include therapeutic exercise into training.
Mid Phase
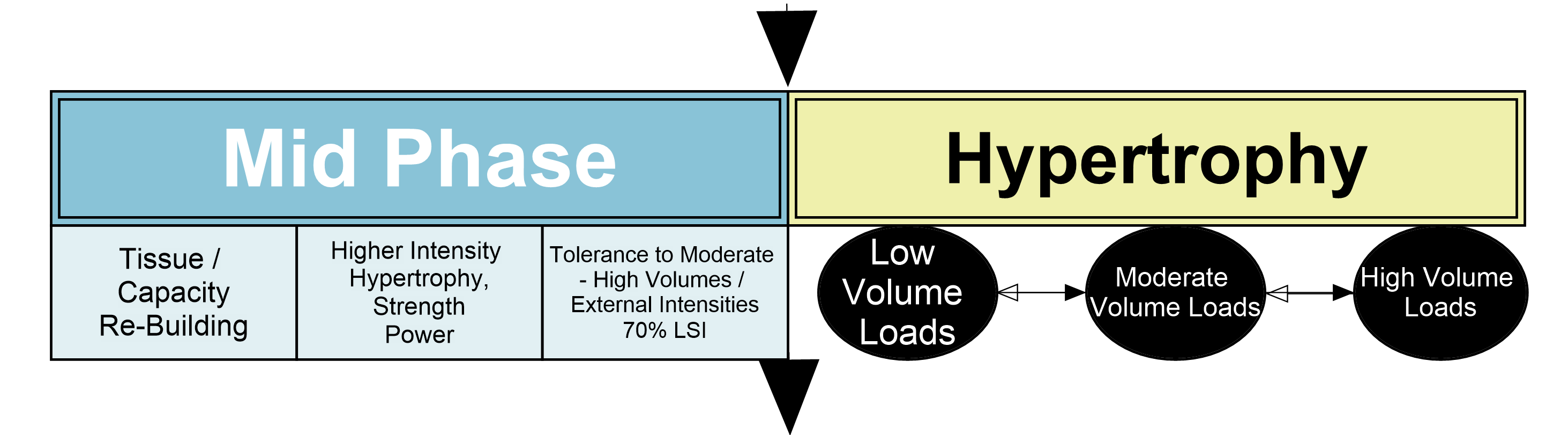
This 3rd phase is the rebuilding phase. Here hopefully for most part the theraband has been put away and instead the tissues are being loaded with implements more specific to the patient’s goals. We are trying to work through a hypertrophy type training continuum for most of our volume with little sprinkles of low volume, higher load (likely constrained by tempo) strength and maybe force absorption work.
By the end of this phase we have been able to show the tissues / system have tolerated moderate levels of mechanical tension / forces for a high volume, and maybe high forces for a low volume. Think daily loading like 2-3 sets 8-15 reps with 3 RIR (repetitions in reserve) compound and isolation exercises involving the tissue and associated kinetic chain. Consider including some initial plyometric preparatory work also.
By the end of this phase we should be doing some functional assessments and the patient should be exceeding 70% LSI to progress. All previous outcomes must also be stable or improving.
Essential communication to stakeholders
- You/they are tolerating rehab / modified training well, tissues are able to safely perform controlled work now.
- You/they are around 70% of the pre-injury level and can likely be involved in low level skill training, running etc.
Mid > Late Phase
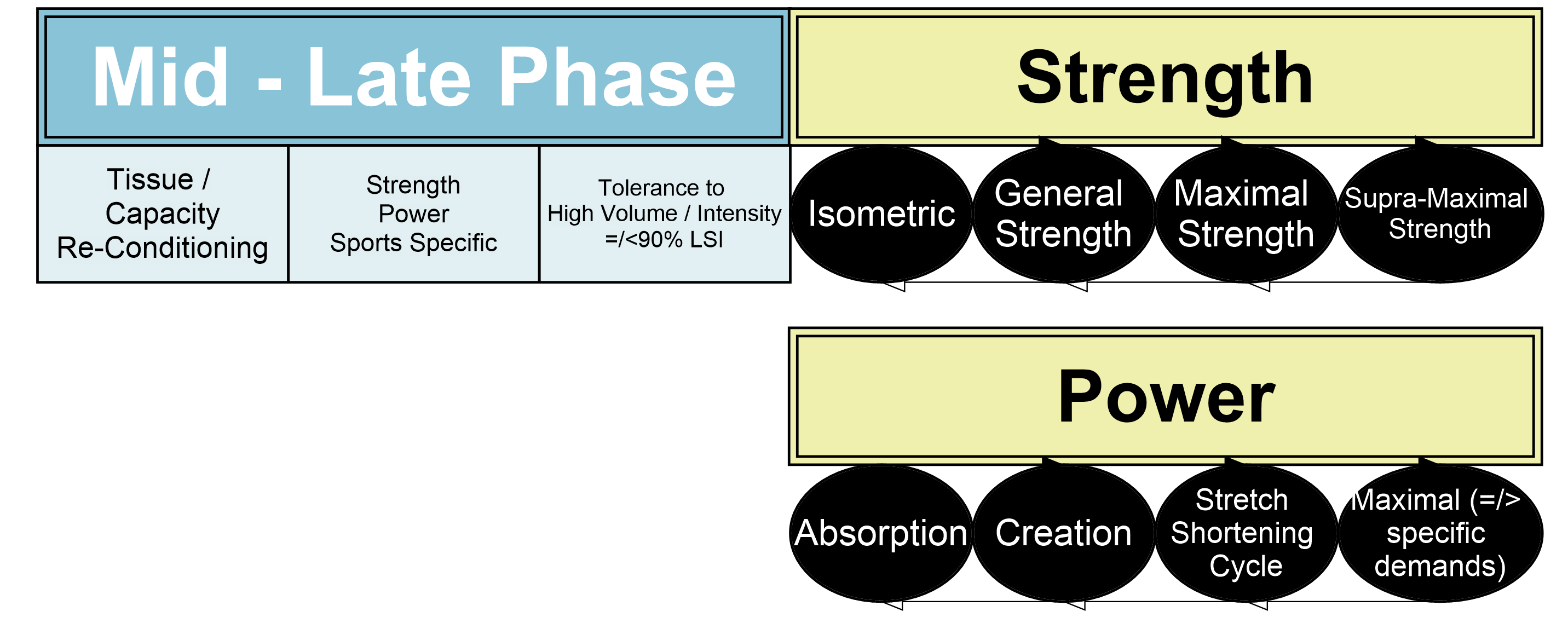
This 4th phase is where things really build up to more specific training for the sport / activity. Most physios would probably feel more confident to hand over the programming reins to an S&C coach at this point, instead taking a consultant role. That is ok if you choose to. There are certain things though we must know to ensure we have objectively assessed tolerance and have a good idea of the patient’s functional capacity to guide risk mitigation conversations.
To exit phase 4 we must be able to show a >90% LSI in the prior assessments, as well as further high level functional tests, and all clinical assessments must be stable. Just as importantly though, we need to be able to tick off tolerance to strength loading through all contraction types and intensities, including the often forgotten supra-maximal / yielding strength (think Nordics), as well as tolerance to the full power and plyometrics continuum. Think 2-3 times per week, 2-5 sets, 2-7 reps, 2-3 RIR of open chain and closed chain strength, power / plyometrics work as appropriate.
Essential communication to stakeholders
- You/they are around 70-90+% of the pre-injury level.
- You/they should be involved in more ‘normal’ training at moderate intensities but low / no level of chaos.
- As the physio you need to objectively see tolerance to the above programming variables to ensure you have done your duty of care mitigate risk to the tissue.
Late Phase / Performance
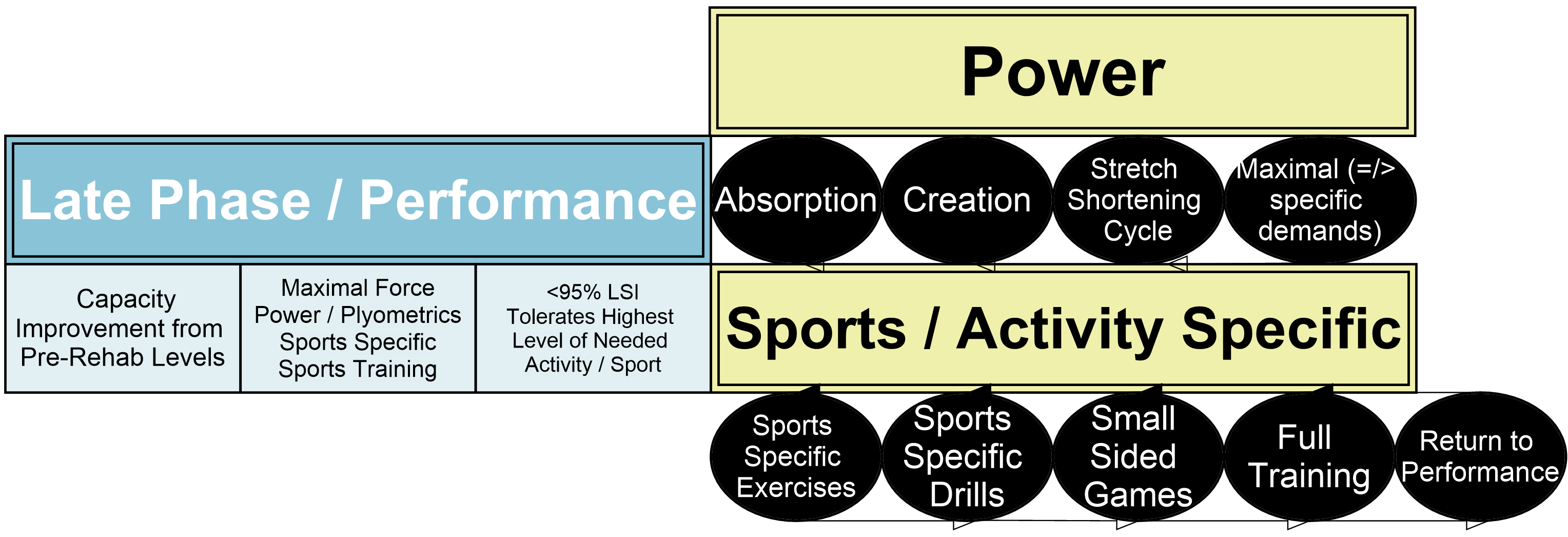
This final phase is characterised by the patient predominantly being involved in their normal training routine. This phase will ramp up from more controlled training environments to more chaotic environments as the patient shows continued tolerance to training (e.g. in team sports – tolerating small-sided games before progressing to full team training; in fitness sports – tolerating weight lifting sessions before met-cons).
The programming in this phase will likely be from external sources, with targeted extra rehabilitation work to catch up to their peers or their unaffected side. As a physio here we will still have to tick off that the patient has tolerated the extra volume of the higher level power and maximal loads equivalent to those that their sport will be putting them under. Tolerance to sport specific training is also a key assessment here.
Think hitting pre-injury numbers on all affected lifts, jumps, running speeds, volumes, accelerations, decelerations etc. The exit criteria here is >95% LSI on all testing above as well as tolerance to an agreed upon number of training sessions at full intensity from all stakeholders.
Essential communication to stakeholders
- You/they are around 95%+ of the pre-injury level.
- The acute risk to tissue re-injury at this stage is low, however risk from relative skill deconditioning in chaotic environments is high until a decent volume of full training has occurred.
- Don’t be afraid to suggest rest days or low volume days here if there are signs of increasing irritability.
- Ensure to get constant feedback from all stakeholders on their thoughts on how the patient is tolerating this phase and book in follow-up appointments to reassess your outcome measures, even if the patient is seemingly doing fine. It is at this time you may pick up on changes to LSI which may indicate negative adaptations.
Conclusion
For a physiotherapist working with active or sporting populations, the above knowledge of strength and conditioning principles and how they affect the tissue being rehabilitated will allow for clear and concise communication around goals, timelines and expectations within the return to sport context. Knowing how to program, or what you are wanting to see out of a program in each phase will mean you can perform your duty of functional capacity assessment and risk mitigation leaving no room for doubt in your decision-making.
Want to learn more about exercise rehab?
Sam Blanchard has done a Masterclass lecture series for us on:
“Clinical reasoning in rehab”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!